This is a writeup of a shallow investigation, a brief look at an area that we use to decide how to prioritize further research.
In a nutshell
What is the problem?
Our impression is that despite the spread of efforts to legalize recreational cannabis use, there is currently relatively little discussion of which legislation models are best for public health. We believe ineffective regulation may carry substantial public health costs.
What are possible interventions?
A philanthropist could fund research into different legalization models and their effects, or could support increased discussion between advocates of cannabis legalization and public health experts with experience in policy related to intoxicants.
Who else is working on it?
A number of foundations do some work on cannabis policy, often within the broader area of drug policy. We are not aware of any major funders who are focusing on designing cannabis policy with a view to protecting public health.
1. What is the problem?
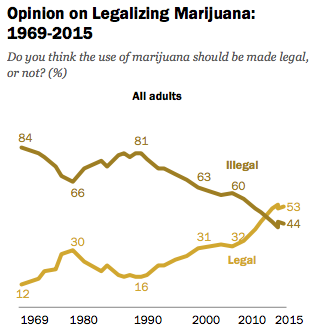
Since 2012, four U.S. states have legalized recreational use and commercial production of cannabis.1 Broadly speaking, we consider it likely that the number of states where recreational cannabis consumption is legal will continue to increase. This view is based on conversations with drug policy experts,2 increased support for legalization in national polls,3 and our general impressions of the current political climate in the U.S.
As discussed below, we believe that different ways of legalizing cannabis use are likely to have widely varying public health implications. In this investigation, we focused on these potential public health effects; we did not thoroughly consider other potential effects of legalization, including (for example) effects on arrests or incarceration. We chose to focus on this aspect because we see the question of how to legalize in a public-health-friendly way as receiving significantly less attention than the question of whether or not to legalize. We see the former question as potentially very important if legalization efforts continue to succeed (which we find likely).
1.1 Public health effects of commercial cannabis production
Our understanding is that the public health impacts of cannabis legalization are likely to depend on the specifics of how legalization is carried out. However, our impression is that relatively little is known about how different kinds of regulatory regimes are likely to affect public health.
We believe that it could be especially important for early-moving states to implement well-designed policy, as we consider it likely that later legalization models will be based on earlier ones (i.e. we expect the form that legalization takes overall to be relatively path dependent). Another consideration in favor of careful policy design early on is that it may be difficult to change existing policies once states have legalized cannabis, especially if, for example, a commercial marijuana industry were to emerge and become established.4
An example of how policy design might affect public health is the extent to which cannabis is allowed to be produced commercially. Legalization models that enable cannabis production to be fully commercialized may cause cannabis prices to drop considerably; we have heard estimates that prices under commercialization might be one tenth or less of current prices.5 Such a price change seems likely to lead to increased consumption of cannabis.
In general terms, we expect increased consumption of intoxicants (like cannabis) to have humanitarian costs both for individuals and for society. In addition, our impression is that cannabis specifically can cause harm in a number of known ways. In this investigation, we focused on cannabis dependence as the main relevant harm. Cannabis dependence is associated with a variety of negative effects, including low energy and motivation; relationship and family problems; financial difficulties; and sleep and memory problems.6
1.2 Size of the problem
As part of our investigation, we estimated how much harm could potentially be averted by well-designed legislation. See footnote for more details of the calculation.7 In summary:
- We assumed that the main harms of sub-optimal legalization would be due to increased cannabis dependence, then used our best guesses of how harmful dependence is, and how much it might increase under full commercialization, to estimate what the difference between well- and badly-designed legislation might be.
- About 18 million people in the U.S. use cannabis at least once per month.
- About 7% of these, or 1.25 million people, meet criteria for what we would consider morally-relevant cannabis dependence (although other sources report 12% have “met criteria for cannabis dependence in the past year”).
- We use an estimated disability weight for cannabis dependence of 0.05 (note that this is lower than the Global Burden of Disease study’s disability weight for cannabis dependence, which is 0.329).
- The estimates we’ve seen suggest that if legalization were accompanied by full commercialization (and therefore much lower prices), cannabis consumption would roughly double.
- We assumed that a doubling in consumption would correspond to a doubling in dependent users.
Combining these figures with a cost of $50,000 per disability adjusted life year (DALY), the cost of full commercialization comes out at roughly $3 billion, although we have very limited confidence in this estimate. This is relatively low compared to our rough estimates of the importance of other cause areas within U.S. policy.
2. What are possible interventions?
We have focused our attention on ways to help cannabis legalization go as well as possible in jurisdictions where it does take place (rather than focusing on affecting the likelihood of legalization itself, which we see as drawing more attention from funders).
Different legalization models could vary along many dimensions, including the following:8
- What type of organizations are allowed to provide cannabis?
- What regulations apply to these organizations?
- What types of products can be sold?
- How much will the products cost?
A funder in this space might consider supporting:
- Research into different legalization models and their effects, e.g. analyzing previous instances of legalization, forecasting the effects of new proposals, or developing new legislative approaches.
- Increased communication between cannabis legalization advocates and public health experts, e.g. holding meetings to discuss different approaches to legalization.
Work of this kind could affect cannabis policy in the short term (e.g. by affecting the language of a specific ballot initiative) or the longer term (e.g. by promoting effective models of regulation which can be adopted more widely in the future, or more generally shifting the discourse around cannabis policy).
3. Who else is working on this?
We do not have a comprehensive picture of which organizations actively support the careful design of cannabis-related policy, as opposed to supporting drug policy reform or cannabis legalization efforts in general. Our impression is that not many groups focus on this aspect of cannabis reform.
The Open Society Foundations (OSF) funds some work on cannabis policy as part of its broader program of domestic drug policy reform but our understanding is that this is not a focus area for OSF.9 A number of other funders, including the Drug Policy Alliance, the Riverstyx Foundation, and the Libra Foundation, fund advocacy around improving drug policy more broadly, but do not focus on cannabis policy specifically as far as we know.10
4. Questions for further investigation
If we were to do further research here, questions we might aim to address include:
- How responsive will legalization advocates be to proposed measures to protect public health?
- What policy designs can best capture the benefits of cannabis legalization while preventing large declines in prices and attendant increases in dependence?
- How does legalizing cannabis affect alcohol consumption patterns and their associated social costs?
5. Our process
We have been interested in this area for several years. We have had many conversations with experts on the topics of criminal justice reform and drug policy reform, some of which have also included discussion of cannabis legalization. Public notes are available from several of these conversations:
- Open Society Foundations, Campaign for a New Drug Policy on November 19, 2012
- Gara LaMarche on May 22, May 31, and June 14, 2013
- Mark Schmitt on May 22 and June 14, 2013
- Mark Kleiman on July 2, 2013
- Mark Kleiman on November 12, 2013
- Andy Ko on November 20, 2013
- Beau Kilmer on January 27, 2015
- Mark Kleiman on February 13, 2015
This area is also a personal interest of Cari Tuna and Dustin Moskovitz, co-founders of the foundation Good Ventures, who have made several personal gifts to support cannabis legalization efforts. Cari and Dustin are members of the Open Philanthropy Project Board of Managers.
The Open Philanthropy Project has made grants to support the following:
- RAND Corporation research on legalization options in Vermont
- A collaboration between the O’Neill Institute for National and Global Health Law at Georgetown University and the Washington Office on Latin America to develop and disseminate a stronger understanding of how different legalization options may affect public health
- Research by Angela Hawken of Pepperdine University on the potential impact of cannabis legalization on use of both cannabis and other illicit drugs
We are not currently planning further grants in this area in the near future, but may revisit the issue once we have a clearer sense of whether these grants have been successful.
6. Sources
| DOCUMENT | SOURCE |
|---|---|
| Budney et al. 2007 | Source |
| Burns et al. 2013 | Source |
| Caulkins 2013 | Source |
| Caulkins 2014a | Source |
| Caulkins 2014b | Source |
| Caulkins et al. 2012 | Source |
| Caulkins et al. 2015 | Source |
| GiveWell’s non-verbatim summary of a conversation with Open Society Foundations, November 19, 2012 | Source |
| Global Burden of Disease Study 2010 | Source |
| Mackin, Martin and McGavin 2007 | Source |
| NIDA – Cocaine, Scope of Use | Source |
| NIDA – DrugFacts, Treatment Statistics | Source |
| NIDA – Marijuana, Is Marijuana Addictive | Source |
| Office of National Drug Control Policy, State Laws Related to Marijuana | Source |
| Our non-verbatim summary of a conversation with Andy Ko, November 20, 2013 | Source |
| Our non-verbatim summary of conversations with Gara LaMarche on May 22, May 31, and June 14, 2013 | Source |
| Our non-verbatim summary of conversations with Mark Schmitt on May 22 and June 14, 2013 | Source |
| Pew Research Center 2015 | Source |
| SAMHSA 2014 | Source |